


ADDRESS TO THE READERS

HEART FAILURE
What is already known about the subject?
- Studies of orthostatic reactions and ambulatory blood pressure (BP) profiles in patients with heart failure (HF) are scarce.
What might this study add?
- ORTHO-HYPO is a specially designed, prospective, multicenter exploratory study within the Cardio-Reno-Hepato-Metabolic Disease in Chronic Heart Failure (CARMEN-CHF) program to examine hypotension patterns in patients with HF based on office BP, orthostatic testing, and 24-hour BP monitoring.
- The study results will help identify key strategies needed to overcome hypotension as a significant barrier to the administration of recommended heart failure therapy in real-world clinical practice.
As part of the observational, multicenter prospective study CardioReno-Hepato-Metabolic Disease in Chronic Heart Failure (CARMENCHF), an additional exploratory study of the types and role of hypotension in heart failure (ORTHO-HYPO) was specifically designed to thoroughly examine hypotension. The study aim is to assess the frequency and types of orthostatic hypotension and orthostatic hypertension and their associations with clinical and demographic characteristics, comorbidity, severity of clinical manifestations of heart failure, and outcomes. In this sub-study, in addition to the routine examination, an active "supine-standing" orthostatic test and 24-h blood pressure and ECG monitoring will be performed.
What is already known about the subject?
- Left ventricular ejection fraction (LVEF) assessment using echocardiography is the most common and accessible method for assessing LV contractility and forms the basis for classifying patients with heart failure (HF).
- Over time, with optimal pharmacotherapy or a recurrent cardiovascular event, myocardial contractility can either improve or worsen, reflecting LVEF changes.
What might this study add?
- Some patients with HF experience an increase or even normalization of LVEF after a baseline decrease. A small proportion of patients with HF and initially preserved LVEF experience a decrease during 3-year follow-up.
- Changes in LVEF during long-term follow-up are an important and accessible marker of prognosis in HF.
Aim. To study the incidence and clinical prognostic significance of changes in heart failure (HF) phenotype based on left ventricular ejection fraction (LVEF) changes over 3 years.
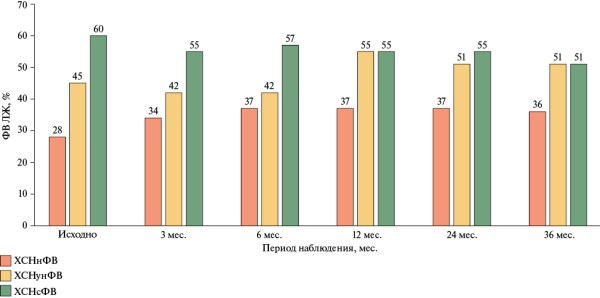
Material and methods. This retrospective study included 157 patients hospitalized with acute decompensated heart failure (ADHF). The results of baseline echocardiography and repeat examinations at 3, 6, 12, 24, and 36 months were assessed. Patients were divided into subgroups based on baseline LVEF as follows: HF with reduced LVEF (HFrEF) (<40%), HF with mildly reduced LVEF (HFmrEF) (40-49%), and HF with preserved LVEF (HFpEF) (≥50%).
Results. Among patients with baseline HFrEF, transition to the HFpEF subgroup was observed in 14%, and transition to the HFmrEF in 20%, while an increase in LVEF >10% was noted in 31% of patients. In the HFmrEF subgroup, LVEF normalized in 48% of patients, and decreased to <40% in 22%. In the HFpEF subgroup, a decrease in LVEF <40% was recorded in 10% of cases. According to the Cox model, the transition from the HFrEF subgroup to the HF with improved EF subgroup was associated with higher overall survival (HR (hazard ratio) 4,57; 95% confidence interval (CI): 1,039-20,177; p=0,04). The risk of cardiovascular death in patients who transitioned from the HFrEF subgroup to any other subgroup (HFmrEF, HFpEF) was also associated with improved survival (HR 8,852; 95% CI: 1,139-68,805, p=0,04). In the HFpEF subgroup, a decrease in LVEF <40% was associated with an increased risk of cardiovascular mortality (HR 4,906; 95% CI: 1,08622,153; p=0,039).
Conclusion. Clinically significant improvement in cardiac function is observed in almost half of patients with a baseline reduced LVEF and is associated with a better prognosis. A decrease in LVEF in the HFpEF subgroup is a predictor of unfavorable outcome.
What is already known about the subject?
- In heart failure (HF), changes in microcirculation were observed in patients with advanced heart failure with reduced or, less commonly, mildly reduced ejection fraction (EF).
- The changes were characterized by a functional rarefaction of capillaries per unit area with an increase in their length and diameter.
What might this study add?
- Approaches to HF classification (division into EF, stages) and its diagnosis that have changed in recent years have made it possible, using a model of patients with stage I-III hypertension with preserved EF, to determine significant changes in microcirculation only in stage I HF in comparison with patients with only HTN and with HTN and pre-CHF.
Aim. To analyze microcirculation in the bulbar conjunctival vessels of patients with stage I-III hypertension and stage 1 heart failure (HF) with preserved ejection fraction (EF) with similar groups of patients with hypertension and pre-HF and hypertension without HF.
Material and methods. One hundred thirty-nine patients with stage I-III hypertension and preserved EF, examined according to the 2024 Heart Failure clinical guidelines, were divided into three following groups: group 1 — patients with hypertension without HF (n=31), group 2 — patients with hypertension and pre-HF (n=19), and group 3 — patients with hypertension and stage I HF (n=89).
Results. The mean arteriolar and capillary diameters, arteriole-to-venule ratio, and number of capillaries per mm2 of conjunctival surface were significantly lower among patients with hypertension and stage I HF compared to groups 1 and 2. No differences in these parameters were found between patients in groups 1 and 2.
Conclusion. In patients with hypertension and an EF ≥50%, significant changes in microcirculation are observed only in stage 1 HF, compared to patients with hypertension alone and with hypertension and pre-CHF. These changes are characterized by a smaller mean arteriolar and capillary diameter, arteriole-venule ratio, and capillaries per mm2 of conjunctival surface.
ISCHEMIC STROKE
What is already known about the subject?
- Stroke is characterized by a high incidence of venous thrombosis.
- Routine early administration of anticoagulants in ischemic stroke is limited by the need to balance the benefits of venous thromboembolism prevention with the bleeding risk.
What might this study add?
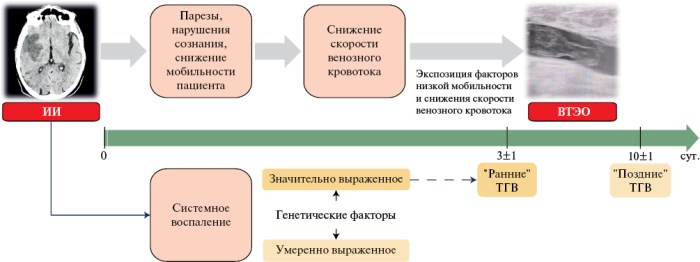
- Systemic inflammation, which is detected in stroke, has a modulating effect on venous thrombosis pathogenesis. High inflammatory activity promotes the development of "early" thromboses (3±1 days). With less severe inflammation, thrombosis is preceded by a longer exposure to the main risk factors.
- The identification of inflammatory markers in ischemic stroke can be considered as an additional justification for the early administration of anticoagulants for the prevention of venous thrombosis.
Aim. To determine the role of systemic inflammation in the development of venous thromboembolism (VTE) in patients with ischemic stroke.
Material and methods. This single-center prospective study included 94 patients with confirmed ischemic stroke and significant mobility impairment (Rivermead Mobility Index ≤3). VTE was diagnosed based on paired ultrasound examinations of the lower extremity veins at 3±1 and 10±1 days of hospitalization and CT pulmonary angiography performed in patients with deep vein thrombosis (DVT). Laboratory markers of systemic inflammation included white blood cell (WBC) count, relative lymphocyte count, relative mid cell count in the complete blood count at admission, leukocyte-lymphocyte ratio, and C-reactive protein levels.
Results. Forty-six (49%) patients were diagnosed with venous thromboembolism (VTE). In 26 cases, DVT was detected by lower extremity vein ultrasound on day 3±1 of hospitalization (early DVT), and in 20 cases, thrombosis was detected on day 10±1 (late DVT). All patients had C-reactive protein levels above reference values on day 3 of hospitalization. An association was established between blood concentrations of inflammatory markers and stroke severity indicators, decreased venous flow velocity, and D-dimer levels. No association was found between systemic inflammation detected during ischemic stroke and underlying chronic inflammatory diseases or acute inhospital infectious complications. Patients with VTE were characterized by significantly more pronounced changes in inflammatory biomarkers. An increase in WBC >12×109/L (area under the receiver operating characteristic curve (AUC) 0,677, p=0,012), a leukocyte-lymphocyte ratio >6,5 (AUC 0,694, p=0,006), and a decrease in the relative lymphocyte content <15% (AUC 0,690, p=0,007) at the time of hospital admission were predictors of early thrombosis.
Conclusion. Ischemic stroke induces a systemic inflammatory response, the severity of which is determined by both the severity of brain injury and the individual characteristics of the patient's inflammatory response. Systemic inflammation has a modulating effect on the pathogenesis of venous thromboembolism (VTE) in patients with ischemic stroke. High inflammatory activity contributes to an earlier (3±1 day) onset of VTE. In patients with moderate inflammation, VTE is preceded by a longer exposure to the main risk factors, and thrombosis develops later (10±1 day). Pronounced inflammatory response in patients with ischemic stroke and significant mobility impairments can be considered as an additional criterion for the early administration of anticoagulants for VTE prevention.
RISK FACTORS FOR CARDIOVASCULAR DISEASES
What is already known about the subject?
- Cardiovascular risk biomarkers are intensively studied to predict the probability of hypertension (HTN) and cardiovascular disease.
- Established risk factors for cardiovascular disease include excess body weight, abdominal obesity, dyslipidemia, poor diet, physical inactivity, stress, smoking, and environmental pollution.
What might this study add?
- Elevated systolic blood pressure in patients with hypertension correlates with excess body weight, regardless of metabolic disorders. However, unfavorable parameters of clinical status (concentric myocardial remodeling, pseudo-normal left ventricular diastolic dysfunction, severity of combined hyperlipidemia, low-density hyperlipoproteinemia) more often develop in patients with hypertension comorbid with metabolic disorders, and are associated with abdominal and general obesity.
Aim. To evaluate the associations of cardiovascular risk biomarkers with clinical status parameters in patients with hypertension (HTN) depending on metabolic disorders.
Material and methods. We studied the associations of clinical status parameters, cardiovascular risk factors, and biomarkers in patients aged 25 to 74 years with HTN with and without metabolic disorders.
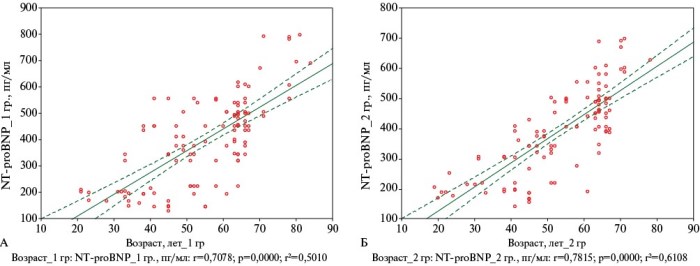
Results. Systolic blood pressure was positively associated with body mass index in both groups (p<0,05). In patients with HTN and metabolic disorders, concentric left ventricular hypertrophy was detected 2,3 times more often (p=0,001), while pseudonormal left ventricular diastolic dysfunction — 2 times more often (p=0,026), heart failure with reduced ejection fraction — 1,3 times more often (p=0,126). Higher values of combined hyperlipidemia were determined compared to patients with HTN without metabolic disorders. The concentration of N-terminal pro-brain natriuretic peptide was not associated with metabolic disorders (p=0,459), and was closely related to age (p=0,001).
Conclusion. In patients with hypertension, elevated systolic blood pressure is associated with excess body weight, regardless of metabolic disorders. Unfavorable indicators of clinical status and structural and geometric cardiac remodeling in patients with HTN and metabolic disorders are associated with abdominal and general obesity.
What is already known about the subject?
- MicroRNAs miR-195-5p, miR-145-5p, and miR-181b-5p are involved in atherogenesis by regulating endothelial dysfunction, inflammation, apoptosis, and vascular remodeling.
- Elevated expression of miR-195-5p is associated with the atherosclerotic progression and vascular calcification.
What might this study add?
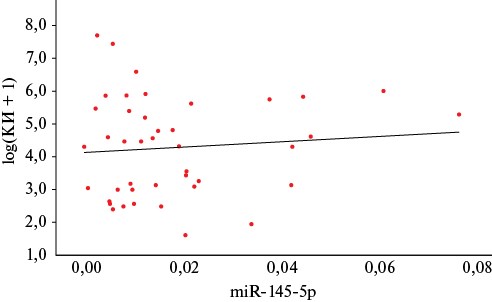
- For the first time, a significant association between reduced circulating miR-145-5p levels and coronary calcification was identified.
- A model using miR-195-5p, miR-145-5p, and miR-181b-5p provided the highest sensitivity for diagnosing early calcification, while a model based on miR-145-5p and clinical parameters was optimal for detecting significant calcification.
Aim. To study the associations of circulating microRNA levels — miR145-5p, -181b-5p, and -195-5p — with coronary artery calcification.
Material and methods. We analyzed data previously collected in a registered database (patent № RU 2024622531). The database is a dbf file (dBSAE IV) and contains 62 unique circulating microRNA profiles from patients at the Clinical Center of the I. M. Sechenov First Moscow State Medical University.
Results. Analysis of the 62 patient database revealed a significant association between reduced circulating miR-145-5p levels and coronary artery calcification, with an Agatston score >0 (p=0,005). In ROC analysis, combined models including miR-145-5p, miR-181b-5p, miR-195-5p and clinical and demographic factors (sex, smoking, nonHDL cholesterol) demonstrated high diagnostic performance as follows: area under the ROC curve (AUC) was 0,85 for detecting any calcification (Agatston score >0), 0,82 for Agatston score ≥10 and 0,84 for significant calcification (Agatston score ≥100). The highest sensitivity (87,2%) and specificity (70%) for an Agatston score ≥10 were achieved using all three miRNAs with covariates, while for an Agatston score ≥100, the model combining miR-145-5p and clinical and demographic parameters was found to be optimal (sensitivity 75%, specificity 90%).
Conclusion. For the first time, a significant association between reduced circulating miR-145-5p levels and calcinosis was identified. Diagnostic models combining the levels of the studied miRNAs with clinical and demographic factors demonstrated high efficiency in identifying various disease stages as follows: the model combining all three miRNAs demonstrated maximum sensitivity for early calcinosis, and the miR-145-5p-based model was optimal for significant calcinosis. Thus, profiling circulating microRNAs, particularly miR-145-5p, represents a promising noninvasive approach for early diagnosis and personalized risk stratification.
What is already known about the subject?
- Elevated lipoprotein(a) levels are a significant genetic risk factor for atherosclerotic cardiovascular disease.
- The low molecular weight apoprotein(a) phenotype is associated with an increased risk of coronary artery disease.
What might this study add?
- Hyperlipoprotein(a) and the low molecular weight apoprotein(a) phenotype are independently associated with stenotic coronary, carotid, and lower extremity artery atherosclerosis, both isolated and in multifocal lesions.
Aim. To study the association between lipoprotein(a) [Lp(a)] and apoprotein(a) [apo(a)] phenotypes with atherosclerosis of various locations and a history of cardiovascular events.
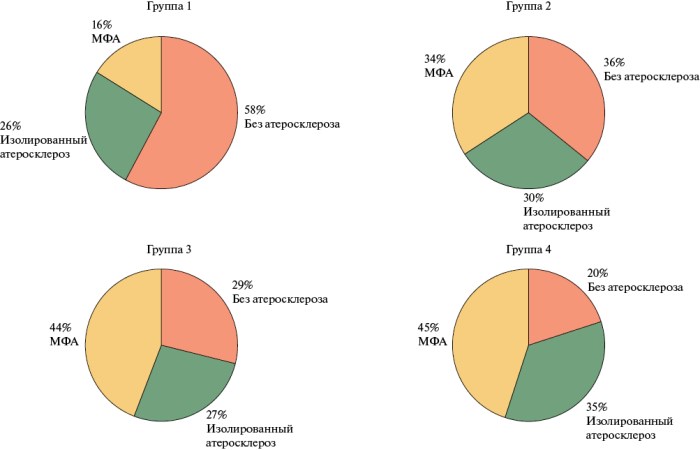
Material and methods. This cross-sectional, single-center study included 819 patients over 18 years of age with available paraclinical data on the coronary, carotid, and lower extremity arteries (LEA). Atherosclerosis was considered significant with stenosis of at least one main artery by more than 50%, as determined by carotid duplex ultrasound, LEA, and coronary angiography. Patients were divided into 4 following groups depending on their Lp(a) level and apo(a) phenotype: group 1 — Lp(a) <30 mg/dL and high-molecular-weight apo(a) phenotype (n=314); group 2 — Lp(a) <30 mg/dL and low-molecular-weight (LMW) apo(a) phenotype (n=122); group 3 — Lp(a) ≥30 mg/dL and high-molecularweight apo(a) phenotype (n=126); group 4 — Lp(a) ≥30 mg/dL and LMW apo(a) (n=257). In all patients, serum lipid and Lp(a) concentrations were determined, and apo(a) phenotyping was performed.
Results. The study groups were comparable by age and sex. In the studied sample, as the concentration of Lp(a) and LMW apo(a) increased from group 1 to group 4, the proportion of individuals without significant atherosclerosis decreased (58, 36, 29 and 20%, respectively), and multifocal atherosclerosis incidence increased (16, 34, 44 and 45%, respectively). LMW apo(a) with Lp(a) <30 mg/dl (group 2) was associated with multifocal atherosclerosis with an odds ratio (OR) of 2,6 (95% confidence interval (CI): 1,6-4,3 (p<0,01)), while hyperlipoproteinemia(a) (Lp(a) concentration ≥30 mg/dL) was associated with a 4-fold increase in the odds of multifocal atherosclerosis (groups 3 and 4) when compared with group 1 — OR 4,0; 95% CI: 2,5-6,4 (p<0,01) and OR 4,0; 95% CI: 2,7-5,9 (p<0,01), respectively. Independent association of Lp(a) and LMW apo(a) levels with atherosclerotic cardiovascular diseases and history of myocardial infarction (MI) was confirmed by logistic regression analysis including age, sex, hypertension, type 2 diabetes, smoking status, and obesity in the model. The odds of coronary, carotid, and multifocal atherosclerosis and history of MI were highest with a combination of hyperlipoproteinemia(a) and LMW apo(a) as follows: OR 4,5; 95% CI: 3,0-6,8 (p<0,01), OR 3,5; 95% CI: 2,2-5,6 (p<0,01), OR 10,9; 95% CI: 5,8-20,5 (p<0,01), OR 2,9; 95% CI: 2,0-4,2 (p<0,01), respectively. No significant association was found between Lp(a) and LMW apo(a) levels with a history of ischemic stroke.
Conclusion. Hyperlipoproteinemia(a) and LMW apo(a) are associated with significant coronary, carotid and LEA atherosclerosis, with isolated and multifocal atherosclerosis and a history of MI, independent of both conventional risk factors and each other. LMW apo(a) was associated with atherosclerotic cardiovascular disease and a history of MI, but not with ischemic stroke, regardless of Lp(a) levels.
What is already known about the subject?
- Adverse behavioral patterns develop at a young age.
- Limited data are available on the prevalence of cardiovascular risk factors among university students.
- The observed worldwide trend is associated with an increasing prevalence of hypertension among young adults.
What might this study add?
- The incidence of identified cardiovascular risk factors among university students is similar to that observed in the adult population, necessitating active preventive measures at an earlier age.
- If young people have a history of high blood pressure, there is a high probability of a combination of unfavorable behavioral factors that multiply their cardiovascular risk, requiring close medical attention.
Aim. To assess the frequency, structure, and combination of cardiovascular risk factors in university students.
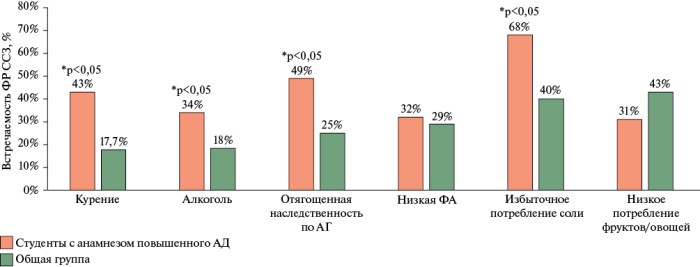
Material and methods. This cross-sectional online survey was conducted among 446 first-year students of a technical university. The questionnaire assessed the following cardiovascular risk factors: smoking, family history of hypertension, low fruit and vegetable consumption, physical activity level, salt intake, and alcohol consumption.
Results. Following unfavorable behavioral risk factors are highly prevalent among first-year university students: low fruit and vegetable consumption (43%), excessive salt intake (40%), and insufficient physical activity (33%). A quarter of these cases are associated with a family history of hypertension.
Conclusion. The online survey is an effective tool for reaching young people and demonstrates a high prevalence of cardiovascular risk factors among students, consistent with previous studies in these cohorts, including large epidemiological data. Young people with a history of high blood pressure require close attention to primary cardiovascular disease prevention, as they are more likely to experience individual risk factors and their combinations.
ENDOVASCULAR INTERVENTIONS
What is already known about the subject?
- Periprocedural myocardial injury (PMI) is one of the most common complications after transcatheter aortic valve implantation (TAVI).
- PMI diagnostic criteria, based on the dynamics of myocardial injury biomarkers, are constantly being revised and refined.
- The short- and long-term prognosis of patients with PMI remains unclear.
- Effective strategies for PMI prevention have not yet been developed.
What might this study add?
- The introduction of novel, improved PMI diagnostic criteria (VARC-3) has led to more stringent verification of the complication. However, the incidence of PMI in TAVI remains clinically significant.
- The diagnostic and prognostic value of key myocardial injury biomarkers (troponin and creatine phosphokinase MB) requires clarification.
- Despite the introduction of VARC-3 criteria to improve risk stratification in a cohort of patients with myocardial infarction who underwent TAVI, short- and long-term prognosis data remain characterized by significant heterogeneity.
Transcatheter aortic valve implantation (TAVI) is an effective minimally invasive treatment for patients with severe aortic stenosis and varying surgical risks. However, like any surgery, TAVI is associated with various complications, including periprocedural myocardial injury. This issue remains understudied, and numerous questions remain unresolved, including not only the diagnosis of periprocedural myocardial injury after TAVI but also the long-term prognosis for patients who experience this complication. This article highlights the following issues related to periprocedural myocardial injury after TAVI: definition, pathogenesis, diagnosis, and its impact on short-term and long-term treatment outcomes.
DIGITAL TECHNOLOGIES AND TELEMEDICINE
What is already known about the subject?
- Convolutional neural networks have found wide application in the analysis of medical images of various formats.
What might this study add?
- The study is unique in the Russian Federation.
- The study results demonstrate the effectiveness of diagnostic models based on artificial intelligence systems when trained on an extremely small sample (the smallest dataset described in the global literature).
Aim. To evaluate the effectiveness of a convolutional neural network trained on an ultrasmall sample for identifying non-modifiable cardiovascular risk factors (sex and age) by digital fundus photographs.
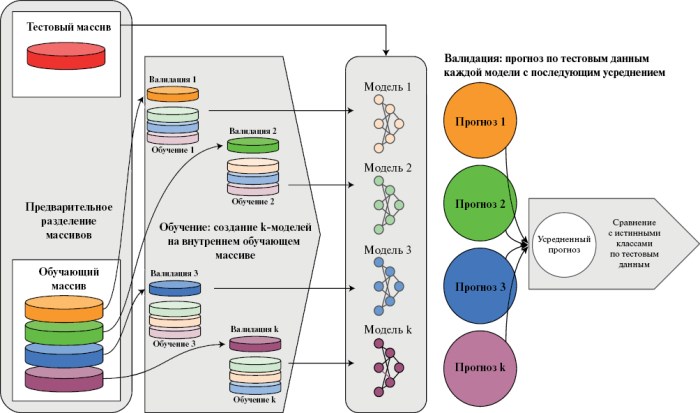
Material and methods. The EfficientNet B3 architecture, pretrained on the ImageNet database, was used. The study was conducted on a proprietary dataset containing digital fundus photographs and patient demographic data, divided into training (227 photos) and test (131 photos) samples. To determine the accuracy of age prediction, the mean absolute error (MAE), the coefficient of determination (R2), and the BlandAltman plots were evaluated. For sex prediction, sensitivity, specificity, positive and negative predictive values, and the area under the ROC curve were assessed.
Results. The MAE for age was 6,04 (95% confidence interval (CI): 5,11-7,11), while R2 — 0,638 (95% CI: 0,486-0,759). The area under the ROC curve for sex prediction was 0,79 (95% CI: 0,70-0,87). Sensitivity, specificity, negative and positive predictive values, and balanced accuracy (at a probability threshold of 0,5) were 88, 58,1, 81,8, 70,1, and 73,2%, respectively.
Conclusion. The obtained results demonstrate high accuracy in sex determination and moderate accuracy in age determination, indicating that acceptable results can be achieved even with a very small dataset.
OPINION ON A PROBLEM
Uncontrolled hypertension (HTN) is one of the leading risk factors for the development and progression of heart failure and cognitive impairment. In real-world practice, up to 75% of patients fail to achieve target blood pressure (BP) levels.
This article summarizes current Russian and international data on the impact of persistent elevated BP on the development of heart failure (HF) and cognitive impairment.
The contribution of uncontrolled HTN can be considered within a "cardiocerebral" continuum — from early, mostly asymptomatic changes to clinically evident conditions. Chronic hemodynamic overload leads to structural and functional myocardial remodeling, diastolic dysfunction and HF progression, as well as involvement to small cerebral vessels with the development of cerebral small vessel disease and cognitive decline. Pre-HF is specifically identified as a stage in which structural changes have already developed but are potentially reversible.
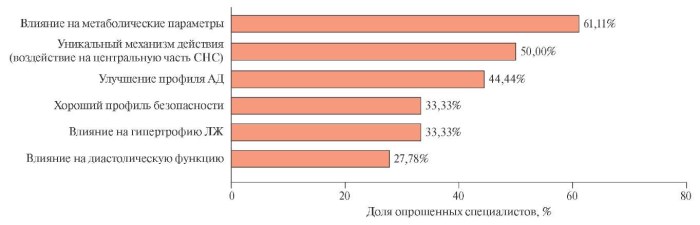
The literature data is supplemented by a survey of specialists, reflecting the specifics of patient management in real-world practice. In their opinion, when treating HTN, in addition to achieving target BP levels, it is necessary to also address comorbid conditions, including metabolic disorders, as well as to implement personalized patient management. In this context, moxonidine (Physiotens®), by reducing sympathetic activity, can be considered as a component of combination therapy in patients with sympathicotonia and concomitant metabolic disorders, ensuring ИЗ control and organ protection.

ISSN 2619-0125 (Online)
















































