


ADDRESS TO THE READERS

CHRONIC HEART FAILURE
What is already known about the subject?
- Heart failure (HF) is associated with a high hospitalization rate. The key molecular pathophysiological processes involved in the development of HF and specifying its severity are chronic low-grade inflammation and programmed cell death.
- Caspases are enzymes involved in programmed cell death processes and play a key role in triggering apoptosis (a non-inflammatory form of cell death) and pyroptosis (an inflammatory form of cell death with release of pro-inflammatory cytokines).
What might this study add?
- Serum caspase-1 levels were shown to be significantly higher in patients with HF than in non-HF individuals.
- An analysis of differences depending on the left ventricular ejection fraction (EF) revealed that the concentration of caspase-8 in HF with reduced EF was 3 times higher than in the group of patients with HF with preserved EF.
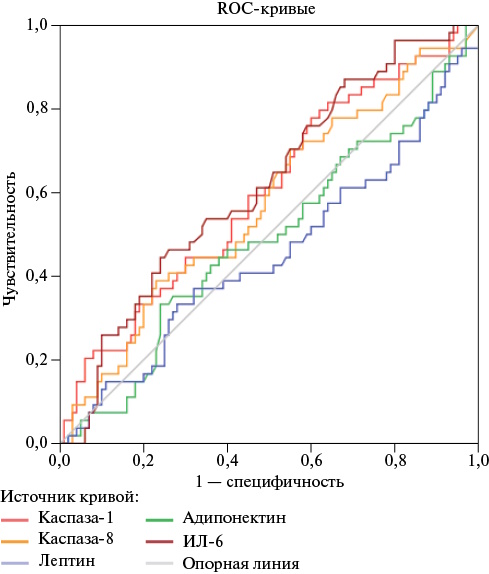
Aim. To conduct a comparative analysis of a complex of programmed cell death biomarkers (caspases-1 and -8, adipocytokines — leptin, adiponectin, and interleukin-6 (IL-6)) in patients with heart failure (HF) and in individuals without this disease.
Material and methods. A total of 154 patients aged 59 to 72 years were examined: 54 patients with HF (study group) and 100 patients without HF (control group). Concentrations of caspases-1, -8, adiponectin, leptin, and interleukin-6 were determined using enzyme-linked immunosorbent assay.
Results. Patients with HF had significantly higher concentrations of caspase-1 and IL-6 than those in the control group. To confirm the potential diagnostic efficacy of the studied biomarkers, a ROC analysis was performed. It showed that when comparing the group of patients with HF and the control group, the highest areas under the curve were characteristic of caspase-1 and IL-6. The median caspase-8 concentration in HF with reduced ejection fraction (HFrEF) 422,2 [139,7-1246,2] pg/ml is 3 times higher than in the group of patients with HF with preserved LVEF — 126,8 [46,8-293,5] pg/ml.
Conclusion. A relationship was found between serum concentrations of caspase-1 and IL-6 and HF, while the concentration of caspase-8 was associated with LVEF and was significantly higher in the subgroup with HFrEF.
What is already known about the subject?
- Myocardial remodeling in most patients with the heart failure (HF) with preserved ejection fraction (HFpEF) phenotype is characterized by concentric hypertrophy and progressive diastolic dysfunction, which are based on myocardial hypertrophy and diffuse fibrosis.
- The main diagnostic/prognostic marker of HF is N-terminal pro-brain natriuretic peptide.
What might this study add?
- Myocardial remodeling in patients with the diabetic phenotype of HFpEF against the background of coronary artery disease and hypertension is characterized by the predominance of eccentric left ventricular hypertrophy, type 2 diastolic dysfunction with pronounced cardiomyocyte apoptosis, activation of proliferative potential and angiogenesis in the myocardium.
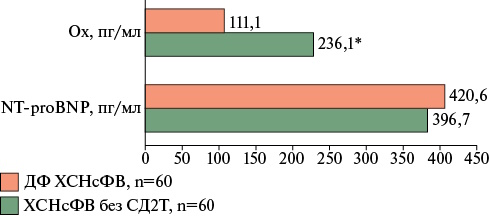
- Low blood oxytocin levels are a distinctive feature of the diabetic phenotype of HFpEF, with a comparable increase in N-terminal pro-brain natriuretic peptide in the general cohort of patients with HFpEF.
Aim. To study novel biomarkers, as well as clinical and morphological features of myocardial remodeling, in patients with the diabetic phenotype (DP) of heart failure with preserved ejection fraction (HFpEF) hospitalized for elective coronary artery bypass grafting.
Material and methods. A total of 120 patients of both sexes with stage I-IIA, class I-III HFpEF (60+60) (with or without type 2 diabetes (T2D)), and underlying coronary artery disease and hypertension were studied. In addition to standard examinations, blood levels of N-terminal pro-brain natriuretic peptide and oxytocin were measured, along with assessment of left ventricular (LV) myocardial remodeling and diastolic dysfunction types. The global LV function index was calculated, and general histological and immunohistochemical (caspase-3, bcl-2, ki- 67, and oxytocin receptors) investigations of right atrial appendage myocardial biopsies were performed.
Results. Myocardial remodeling in DP of HFpEF was characterized by the predominance of eccentric hypertrophy (43%), type 2 diastolic dysfunction (p=0,028), lower LV ejection fraction (p=0,002), and lower LV global function index (p=0,042) compared to patients without T2D. The morphological profile of the myocardium in DP of HFpEF demonstrated significant activation of angiogenesis (p=0,006), apoptosis (p<0,001), and proliferative potential of cardiomyocytes (p=0,049). The identified changes were accompanied by a significant decrease in blood oxytocin level (p<0,001) and high expression of oxytocin receptors (p<0,001) in the myocardium of patients with DP of HFpEF compared to the group without T2D.
Conclusion. A distinctive feature of the myocardial remodeling marker panel in patients with HFpEF in this study was a low blood oxytocin level and a high cardiomyocyte apoptosis index.
ISCHEMIC HEART DESEASE AND MYOCARDIAL INFARCTION
What is already known about the subject?
- Patients who have had a myocardial infarction with underlying heart failure often experience anxiety and depression, which worsens their prognosis.
- Standard cardiac rehabilitation does not always improve psychological well-being. Intermittent hypoxia-hyperoxia training (IHHT) improves cardiovascular function, but its impact on mental status and quality of life has been poorly studied.
What might this study add?
- In elderly patients after myocardial infarction with underlying heart failure, the addition of IHHT to standard rehabilitation significantly reduced anxiety, improved quality of life, and improved exercise tolerance compared to standard rehabilitation alone.
- IHHT is safe and well-tolerated, offering a comprehensive rehabilitation tool.
Aim. To study the effect of rehabilitation using intermittent hypoxia-hyperoxia training (IHHT) on anxiety and depression, quality of life (QOL), and exercise tolerance in elderly patients with myocardial infarction (MI) and heart failure (HF).
Material and methods. This single-center, prospective, randomized, controlled, parallel-group study included 102 elderly patients with MI and HF. Patients were randomized into two groups: the experimental group (n=51) received standard rehabilitation combined with IHHT using the ReOxy device; the control group (n=51) received standard rehabilitation alone. All patients were assessed for anxiety and depression using the Hospital Anxiety and Depression Scale (HADS), quality of life using the EuroQol-5D questionnaire, and 6-minute walk test distance.
Results. The groups were comparable in clinical and demographic characteristics (p>0,05). In the experimental group, compared with the standard rehabilitation group, there was a more pronounced decrease in the HADS score (2,0 (0,0; 7,0) vs 1,0 (0,0; 4,0), p=0,040) and an improvement in QOL according to the European Quality of Life 5 Dimensions 5 Level Version (EQ-5D-5L) visual analogue scale (20,0% (0,0; 30,0) vs 15,0% (-25,0; 30,0), p=0,044). This was accompanied by a greater increase in distance during the 6-minute walk test (up to 51,0 (33,0; 86,0) m in the experimental group vs 30,0 (22,5; 56,0) m, p=0,001).
Conclusion. Adding IHHT to a standard rehabilitation program for patients with MI and HF reduces anxiety, improves QOL, and improves exercise tolerance.
What is already known about the subject?
- Cardiogenic shock remains the leading cause of inhospital mortality in myocardial infarction.
- Myocardial reperfusion and microcirculation specify prognosis, but clinical and angiographic predictors of outcome are poorly understood.
What might this study add?
- For the first time, it has been shown that in cardiogenic shock developing in the first 48 hours after myocardial infarction, type 2 diabetes and higher systolic blood pressure on admission are independent predictors of inhospital death.
- Achieving optimal angiographic results (Thrombolysis In Myocardial Infarction 3) is associated with a significant protective effect.
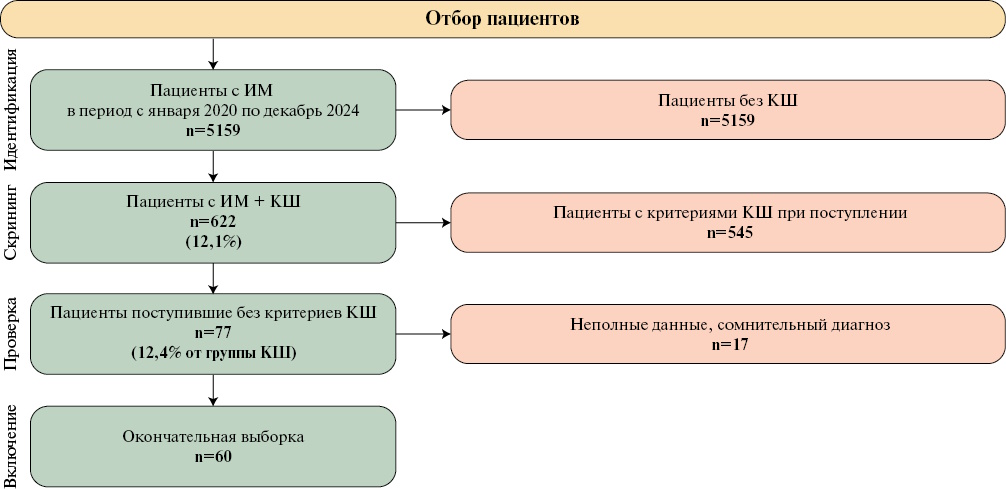
Aim. To evaluate the clinical, hemodynamic, and paraclinical characteristics of patients with myocardial infarction (MI) who developed stage B or higher cardiogenic shock (CS) within 48 hours of admission in the absence of shock signs at admission, and to identify factors associated with mortality.
Material and methods. This retrospective analysis included 60 patients. The primary endpoint was inhospital death. Univariable and multivariable logistic regression analyses were used.
Results. Mortality in this cohort of patients was 55%. Independent predictors of mortality in the multivariable model were type 2 diabetes (odds ratio (OR) 149,6; p=0,001) and higher systolic blood pressure on admission (OR 1,08 per 1 mm Hg; p=0,015). Furthermore, achieving optimal reperfusion (Thrombolysis In Myocardial Infarction (TIMI) 3 was an independent protective factor (OR 0,009; p=0,015). The area under the ROC curve for the model was 0,70.
Conclusion. In patients with MI followed by CS, signs of Society for Cardiovascular Angiography and Interventions (SCAI) stage A may be detected already upon admission. These parameters have prognostic significance and can be used for early mortality risk stratification and selection of monitoring strategies.
КАРДИООНКОЛОГИЯ
What is already known about the subject?
- As survival rates for cancer patients improve, the need for prevention and timely treatment of complications associated with anticancer therapy increases.
- Due to the steady increase in the use of immune checkpoint inhibitors (IPIs), studying the prevalence and mechanisms of immune-mediated complications is becoming increasingly important for the development of primary prevention models.
What might this study add?
- This study demonstrated a high incidence of cardiovascular complications associated with IPI therapy, emphasizing the importance of cardiac monitoring in this group of patients, with echocardiography playing a key role.
- Data supports the use of the echocardiographic left ventricular myocardial performance index and body mass index in the basic risk stratification of cardiovascular complications, which requires further validation.
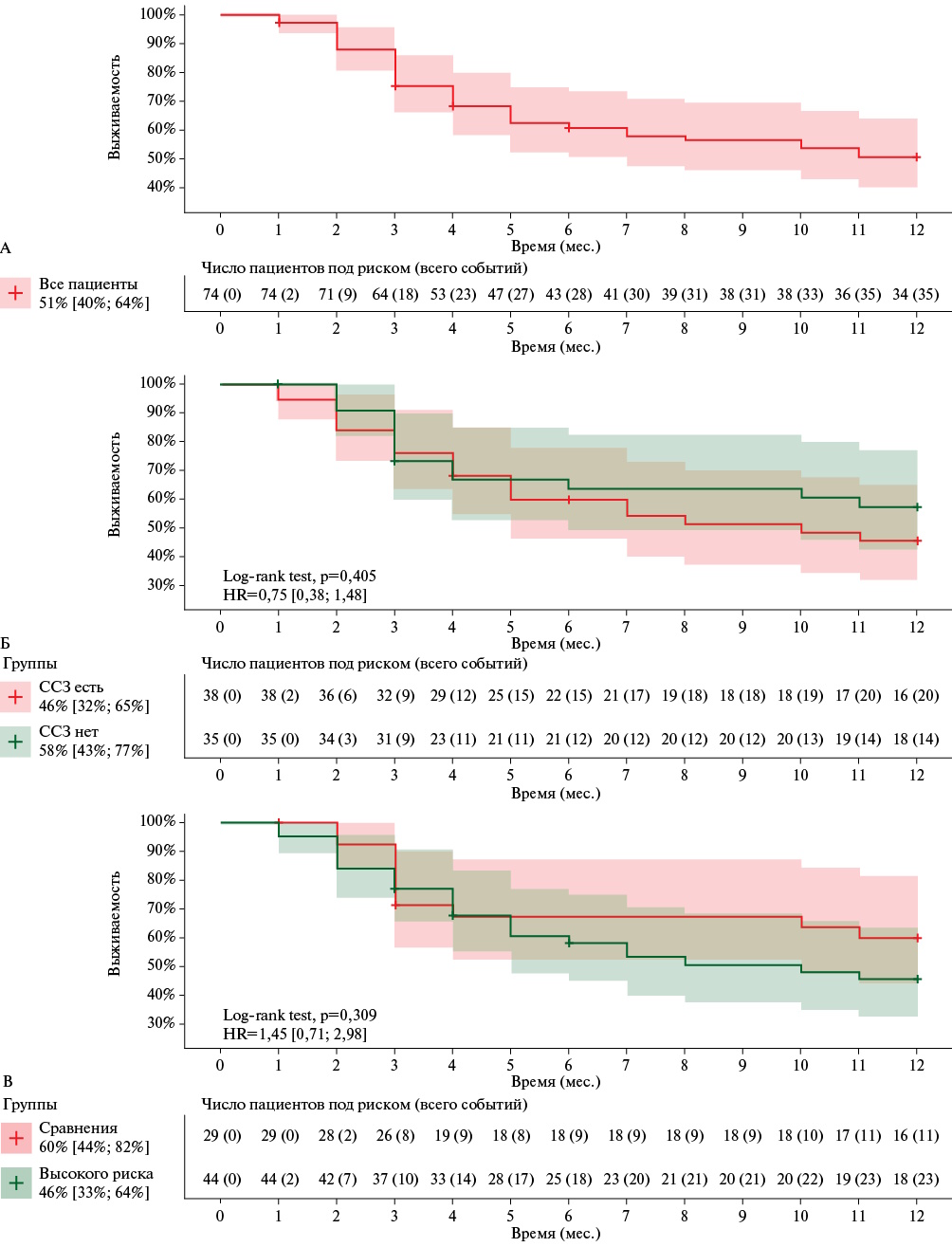
Aim. To assess the incidence of cardiovascular complications associated with immune checkpoint inhibitor (ICI) therapy and identify potential predictors.
Material and methods. The study included 82 patients receiving anticancer treatment with ICIs. Patients were examined before initiation of anticancer therapy (point 0), and at 3 (point 1), and 9 (point 2) months after initiation. The total follow-up period was 12 months. Laboratory parameters, including troponin I, N-terminal pro-brain natriuretic peptide, and markers of atherosclerosis progression (oxidized low-density lipoprotein and heat shock protein), were assessed at all points. All patients underwent echocardiography to assess left ventricular (LV) myocardial strain parameters, carotid ultrasound, and 24-hour electrocardiogram monitoring.
Results. Overall 12-month survival was 51% [40; 64], with no differences between patients with and without underlying cardiovascular disease (46% vs 58%; p=0,405). Clinically insignificant increases in ascending aorta diameter (p=0,040), left atrial size (p=0,16), left atrial volume (p=0,036), and end-systolic volume (p=0,038) were observed, as well as a decrease in LV ejection fraction (p=0,022). No significant changes in cardiac marker levels were observed during the follow-up period. Moreover, the following were identified as predictors of fatal outcomes: initial increase in troponin I level >3,5×10-3 pg/ml (odds ratio, OR: 2,6, 95% confidence interval: 1,3-5,4, p=0,001) and N-terminal pro-brain natriuretic peptide >134,8 pg/ml (OR: 2,4, 95% confidence interval: 1,1-5,3, p=0,038). A high frequency of cardiovascular events of 18,3% (n=15) was revealed. The main predictors of new non-thromboembolic cardiovascular events were a body mass index <20,5 kg/m2 (hazard ratio (HR): 4,2 [1,1; 17,2], p=0,041) and an echocardiographic LV myocardial performance index >0,5 (HR: 10,7 [1,3; 86,5], p=0,026).
Conclusion. A high incidence of cardiovascular complications with ICI therapy was demonstrated, regardless of underlying cardiac pathology in patients. Data support the use of the echocardiographic LV myocardial performance index and body mass index in the basic risk stratification of cardiovascular complications with ICI.
ATHEROSCLEROSIS
What is already known about the subject?
- Inflammatory bowel disease (IBD) increases the risk of atherosclerotic cardiovascular disease, despite a lower prevalence of traditional risk factors.
- Data on the influence of sex on the risk of cardiovascular disease in patients with IBD are inconsistent.
What might this study add?
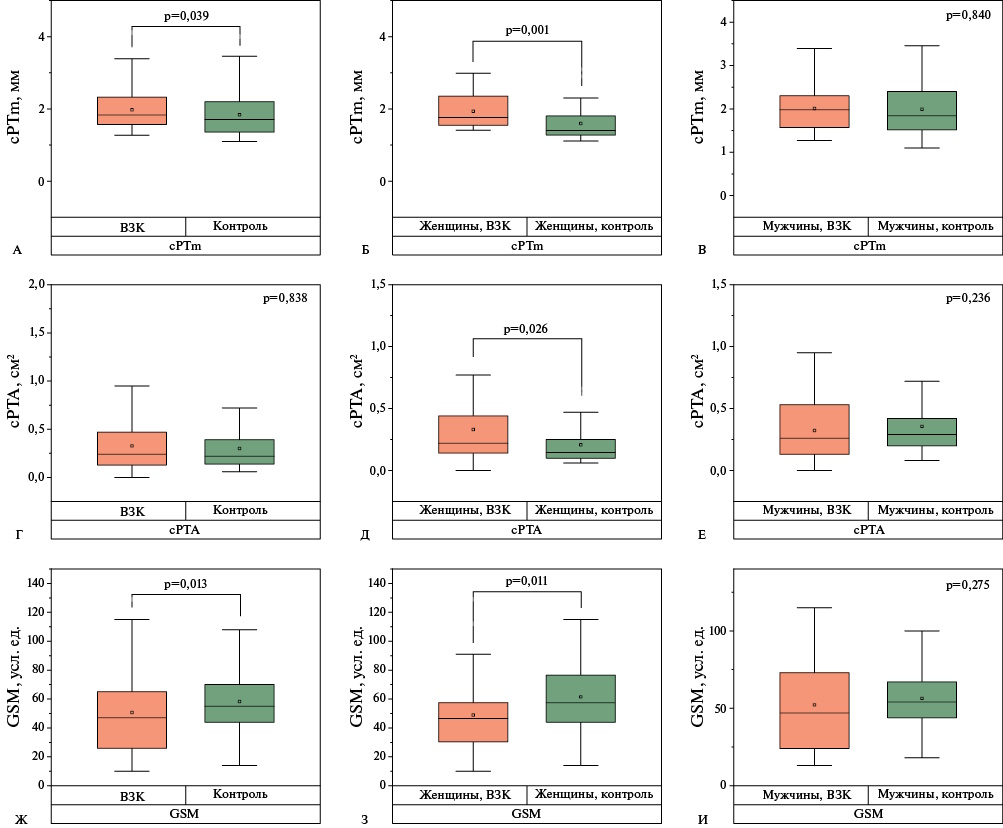
- Women with IBD and carotid atherosclerosis are characterized by lower echogenicity of carotid plaques and higher atherosclerotic burden compared with age-matched controls.
- A diagnosis of IBD was associated with an increased odds ratio for hypoechoic carotid plaques in a model adjusted for age, obesity, smoking, hypertension, low-density lipoprotein cholesterol, triglycerides, glucose, and lipid-lowering therapy among women only.
Aim. To study the influence of sex on the ultrasound plaque morphology and the burden of atherosclerosis in patients with inflammatory bowel disease (IBD) and carotid atherosclerosis.
Material and methods. This case-control study included 59 patients (28 women and 31 men) aged 40-64 years with IBD and carotid atherosclerosis. The control group (n=149, 56 women and 93 men) was recruited from a database of patients with carotid plaques. All patients underwent carotid duplex ultrasound to determine plaque echogenicity and measure the maximum height, total height, and total area of plaques.
Results. The carotid plaque echogenicity was significantly lower in women with IBD compared to the control group (p=0,011). The maximum and total heights of carotid plaques, as well as the total area of carotid plaques, were higher in women with IBD compared to the control group (p=0,001; p=0,003; p=0,026, respectively). IBD in women was associated with a 4,14-fold increase in the odds ratio of hypoechoic carotid plaques (95% confidence interval: 1,11-15,5; p=0,035) after adjusting for age, obesity, smoking, hypertension, low-density lipoprotein cholesterol, triglyceride, glucose levels, and lipid-lowering therapy.
Conclusion. Women with IBD had lower echogenicity of carotid plaques and higher carotid atherosclerosis burden scores compared with age-matched controls. IBD is associated with an increased probability of hypoechoic carotid plaques among women.
RISK EVALUATION
What is already known about the subject?
- Increased breast fat may serve as a specific marker of cardiovascular risk in women, regardless of their body mass index.
- Low breast density and the presence and prevalence of breast calcifications based on screening mammography are associated with higher cardiovascular risk (CVR) in women over 40 years of age.
What might this study add?
- For the first time in women representing the Russian population, we demonstrated that CVR assessment based on screening mammography can serve as a basis for determining subsequent patient routing within outpatient screening.
- Five cardiovascular risk groups have been identified, each with significant differences in CVR levels, taking into account multiple comparisons.
- A step-by-step algorithm for CVR assessment has been developed, potentially suitable for use in clinical practice.
Aim. To evaluate quantitative digital mammography parameters and develop an integrated cardiovascular risk (CVR) assessment system based on these parameters in women over 40 years of age.
Material and methods. This retrospective study assessed mammograms from 1029 patients aged 40 to 75 years, for whom data were available to assess CVR. The mammographic parameters studied were breast density and calcifications. The data needed to assess the CVR were obtained from the medical records of patients receiving outpatient care. CVR was defined as low, moderate, high, and very high in accordance with the Russian Society of Cardiology guidelines.
Results. Quantitative assessment of parameters obtained during preventive mammography allows us to divide patients into five groups with different probability of high and very high CVR. Using univariate logistic regression, odds ratios were calculated for each group compared to the reference value (D0). In groups D1, D2, D3, and D4, the odds of having stage 3-4 CVR were greater than 2,1, 3,5, 4,9, and 13,8 times, respectively. Similar or alternative algorithms for assessing CVR based on preventive mammography data have not been described in the literature.
Conclusion. The development of a step-by-step cardiovascular risk assessment algorithm, potentially suitable for clinical practice, will significantly facilitate and accelerate identifying high cardiovascular risk in women over 40 years of age without the use of invasive diagnostic methods.
What is already known about the subject?
- The influence of physiological mechanisms of adaptation to extreme cold and heat on hemodynamics has been fairly well studied, but much less is known about the influence of atmospheric pressure.
What might this study add?
- The structure of lags between the impact of changing weather conditions and the response of hemodynamic parameters has been studied for the first time.
- We showed that the effect of extreme temperatures on hemodynamics is more pronounced than the effect of extreme atmospheric pressure.
- Sharp 24-hour changes in atmospheric pressure and extremely low atmospheric pressure are statistically associated with increased blood pressure, while high atmospheric pressure is not a risk factor for hypertension.
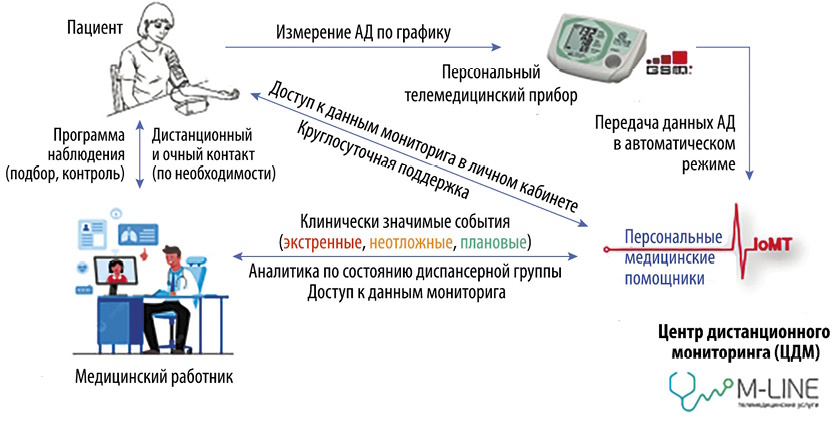
Aim. To assess the impact of heat waves, cold waves, extremely low and high atmospheric pressure, and 24-hout fluctuations in atmospheric pressure on blood pressure (BP) and heart rate (HR) in patients with hypertension (HTN) using remote BP and HR monitoring in various regions of the Russian Federation.
Material and methods. The analysis of the database of the multicenter prospective study "Assessment of the clinical and economic effectiveness of remote monitoring of patients with hypertension" was conducted as part of the implementation of strategic socio-economic initiative "Personal Medical Assistants". The study included patients with HRN over 18 years old, receiving antihypertensive therapy and living in Tyumen (n=1374), Novosibirsk (n=428) and Surgut (n=548). BP and HR were measured in the morning and evening. Follow-up was conducted from November 14, 2023, to December 23, 2024. The influence of meteorological factors on the averaged 24-hour values of the indicator studied was assessed in two stages using the method of time series analysis with 24-hour resolution. In the first stage, "local effects" were calculated in each city, numerically characterizing the influence of a given stress factor on the physiological indicator under study, using a linear generalized regression model of mortality. In the second stage, random-effects meta-analysis was used to obtain pooled effect estimates.
Results. During heat waves, there was a decrease in BP with the magnitude of the effect gradually decreasing with increasing lag and maintaining statistical significance until day 11. During cold waves, an increase in blood pressure was observed, with the magnitude of the effect also decreasing with increasing lag and maintaining statistical significance until day 3. In absolute terms, the effect of heat is 2-3 times greater than that of cold, reaching 3,5 mm Hg for systolic blood pressure. Extremely low atmospheric pressure and particularly sharp pressure fluctuations during the day are risk factors, leading to increased blood pressure and heart rate. However, the absolute magnitude of the effect is quite small, not exceeding 0,8 mm Hg for systolic blood pressure.
Conclusion. The study results confirmed the influence of meteorological factors on the hemodynamics of hypertensive patients, even those receiving antihypertensive therapy. Further study of the influence of meteorological factors on blood pressure and heart rate is of great practical importance.
BIOBANKING

What is already known about the subject?
- The role of a biobank in medical research center functioning is demonstrated.
- Methods for forming a collection of pathogenic, opportunistic, and probiotic microorganisms are described.
What might this study add?
- The results of creating a collection of microbial cultures isolated from biomaterials obtained from proctological patients with inflammatory bowel disease, Crohn's disease, anastomotic leakage, and other gastrointestinal diseases are presented.
This article examines key aspects of the structural organization and functioning of a biobank, including the main stages of biological sample processing. Particular attention is paid to the implementation of research projects using preserved biological material and microbial strain collections. The article describes collection of microorganism strains and biological material in a cryobank, a division of the reference center for the verification of microbiological research results in coloproctology, established at the A. N. Ryzhikh National Medical Research Center of Coloproctology. This article presents the experience of a reference center collaborating with medical facilities in Russian regions within the biological risk monitoring system. A cryobanking system for samples in priority areas of biomedical research is described. The obtained results demonstrate the importance of an integrated approach to biobanking for improving the effectiveness of scientific and clinical developments.
CLINICAL CASES

- Breast arterial calcification and diffuse idiopathic skeletal hyperostosis share common risk factors with cardiovascular disease — age, hypertension, type 2 diabetes, and hyperlipidemia.
- Both conditions are associated with tissue calcification; however, the mechanisms underlying these pathological conditions appear to be different.
- Both breast arterial calcification and diffuse idiopathic skeletal hyperostosis are associated with an increased risk of cardiovascular disease, which requires efforts to identify asymptomatic forms of other noncommunicable diseases.
Introduction. Diffuse idiopathic skeletal hyperostosis (DISH) is excessive bone formation and ligamentous ossification associated with male sex, age, metabolic factors (obesity, diabetes), thoracic aortic calcification, and an increased risk of coronary artery disease. Breast arterial calcification (BAC) is currently considered a marker of cardiovascular risk in women, as numerous studies have demonstrated an association between BAC and coronary artery disease, ischemic stroke, and cardiovascular mortality. The prevalence of both DISH and BAC is approximately 10%, so the combination of these two pathological conditions in this patient is of clinical interest.
Brief description. A 49-year-old woman was diagnosed with suspected DISH during a routine chest X-ray, and moderate BAC was also detected for the first time. Three years later, the patient was invited to participate in a research program. On examination, there are no limitations in mobility in any part of the spine. There was class 2 obesity. Thoracic spine radiography reveals calcification of the anterior longitudinal ligament with features characteristic of DISH. Magnetic resonance imaging of the lumbosacral spine and sacroiliac joint reveals no extension of the ossification process to other spine parts except the thoracic region. Blood tests reveal no signs of inflammation, calcium metabolism disorders, dyslipidemia 2a, and a negative HLA-B27 test, which also supports the diagnosis of DISH. Repeat mammography revealed the BAC progression.
Discussion. When both DISH and BAC are detected, it is important to consider that both these conditions are associated with a significant increase in cardiovascular disease risk. Therefore, it is important to pay attention to the patient's existing risk factors and focus efforts on their correction and the identification of asymptomatic forms of other noncommunicable diseases.

- A patent foramen ovale can cause ischemic stroke.
- Serious complications of endovascular closure of a patent foramen ovale are rare, therefore their exact rate is unknown, and treatment strategies have not been developed.
- A case demonstrates intraoperative ST segment elevation, which could have been caused by an air embolism.
- As a preventative measure, the delivery system should be flushed until air bubbles disappear.
Introduction. The complication rate of endovascular patent foramen ovale (PFO) closure is considered low. However, for most of complications, the rate has not been precisely determined. The most serious intraoperative complications include damage to the heart wall and vessels with bleeding, malpositioned occlude device, thromboembolism, and air embolism. Reports of severe and potentially fatal complications are rare, making their consideration and the determination of treatment strategies crucial.
Brief description. Patient K. aged 36 years had an ischemic stroke. Examination revealed a PFO with significant bypass grafting. Endovascular closure of the PFO was recommended to prevent recurrent ischemic events. During surgery, ST segment elevation was recorded in leads II and III. Selective coronary angiography revealed no contrast enhancement in the distal posterolateral and posterior descending arteries. Intracoronary nitroglycerin was administered, which restored flow in the artery. After the patient's condition stabilized, endovascular closure of the PFO was successfully completed, and an occluder was implanted.
Discussion. Possible causes of intraoperative ST segment elevation include gas embolism from air bubbles remaining in the delivery system after flushing, and mechanical irritation of the interatrial septum. Preventive measures include thorough flushing of the delivery system and selection of the occluder size based on heart anatomy.

ISSN 2619-0125 (Online)
















































