


МЕТАБОЛИЧЕСКИЕ НАРУШЕНИЯ
What is already known about the subject?
- Metabolic-associated fatty liver disease, within the structure of metabolic syndrome, is an independent factor in coronary artery disease and increased cardiovascular risk.
What might this study add?
- The combination of myocardial infarction and metabolic-associated fatty liver disease is characterized by persistently elevated transaminase levels and high epicardial fat thickness values.
- A predominant association between steatohepatitis and greater epicardial fat thickness and aminotransferase levels has been demonstrated in ST-elevation myocardial infarction.
Aim. To assess the relationship between epicardial fat thickness (EFT) and metabolic-associated fatty liver disease (MAFLD), including hepatic steatosis (HS) and steatohepatitis, in myocardial infarction (MI), as well as to analyze the changes of transaminase levels in patients with a combination of ST-elevation MI (STEMI) and MAFLD to accurately identify liver disease.
Material and methods. A total of 163 patients with ST-elevation myocardial infarction (STEMI) (n=144) and non-ST-elevation myocardial infarction (NSTEMI) (n=19) with metabolic syndrome (MetS) were admitted for primary coronary angiography and percutaneous intervention (PCI). Eighty-two patients had concomitant MAFLD (55 with steatosis and 27 with steatosis). Liver elastometry, EFT measurement, cardiac troponin I levels, alanine and aspartate aminotransferase (ALT and AST) levels, and cytokeratin-18 fragment concentrations were measured.
Results. MAFLD in patients with MI compared to patients without liver pathology is associated with higher EFT (p<0,01). According to two-way analysis of variance, a stable increase in blood AST and ALT levels was established for the combination of MI and MAFLD (p<0,05, generalized η² effect size ≥0,11 for both aminotransferases). In STEMI combined with steatohepatitis, compared to HS and STEMI without MAFLD (control), a significantly higher EFT (p<0,01), AST (p<0,05) and ALT (p<0,001) levels were noted.
Conclusion. MAFLD in patients with MI is associated with an increase in EFT. For the combination of STEMI-steatohepatitis, compared to STEMI-HS and STEMI without MAFLD, a higher EFT was observed. This may indicate not only the role of EFT in acute coronary pathology but also the relationship of this indicator with MAFLD severity. In uncomplicated STEMI, analysis and interpretation of transaminase activity in assessing MAFLD are recommended no earlier than 10 days.
What is already known about the subject?
- Excess accumulation of abdominal adipose tissue, regardless of body weight, leads to insulin resistance (IR).
- Magnetic resonance imaging to quantify visceral fat is a current trend at the intersection of radiology, cardiology, and diabetology.
What might this study add?
- A relationship between IR and fat volume was demonstrated, depending on the severity of IR and the presence of metabolic syndrome.
- Associations between visceral obesity and metabolic syndrome were identified in individuals with chronic coronary artery disease.
Aim. To evaluate the association between abdominal fat distribution and metabolic score of insulin resistance (IR) — Mets-IR, depending on the presence of metabolic syndrome (MS) in patients with stable coronary artery disease (CAD).
Material and methods. Sixty-one patients with chronic CAD. The significance of coronary atherosclerosis was determined using the Gensini Score. MS was defined according to the International Diabetes Federation criteria (2005). Abdominal magnetic resonance imaging (MRI) was performed at the L4-L5 level to determine the volume of abdominal fat depots. Blood glucose and insulin levels, lipid profile parameters, and adipokines were determined. Insulin resistance was assessed by calculating the homeostatic model assessment of IR (HOMA-IR) and Mets-I R.
Results. The MS group had significantly higher body mass indices and waist circumference, and between-group differences were found in glucose, serum leptin, and Mets-IR levels. In the MS group, abdominal subcutaneous adipose tissue (SAT) and visceral adipose tissue (VAT) showed a strong correlation with Mets-I R. Patients with severe IR were characterized by increased VAT and SAT volumes; no difference in the VAT/SAT ratio was found. Body mass index, waist circumference, serum glucose, triglyceride, and high-sensitivity C-reactive protein levels were significantly higher, while high-density lipoprotein cholesterol levels were lower with greater IR severity.
Conclusion. The relationship between IR and abdominal adipose tissue volume varies depending on the severity of IR and differs depending on the presence of metabolic syndrome. Among individuals with chronic coronary artery disease (CAD), abdominal visceral obesity is associated with metabolic syndrome. The use of Mets-IR has demonstrated its validity in assessing IR in patients with CAD and metabolic syndrome, as well as a strong association with magnetic resonance imaging (MRI) parameters of abdominal fat depot volume.
ENDOVASCULAR INTERVENTIONS
What is already known about the subject?
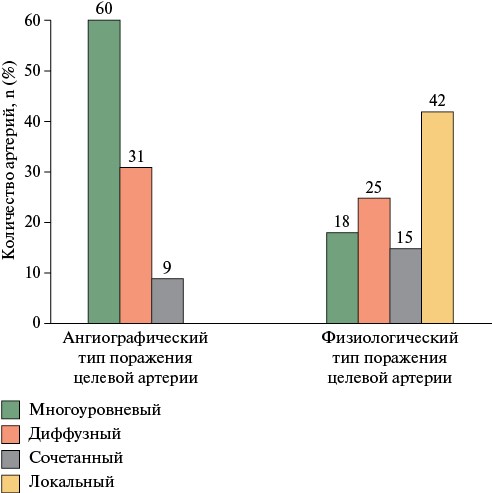
- Diffuse and multilevel atherosclerosis account for ~25% of all percutaneous coronary interventions (PCI) in patients with stable coronary artery disease and are independent predictors of poor long-term prognosis.
- Myocardial revascularization in this group of patients may depend on determining the functional significance of each individual stenosis, which remains an unresolved diagnostic challenge in practice.
- A relatively new method of iFR-guided "virtual stenting" assesses the functional significance of individual lesions and the prediction of potential changes in iFR after PCI, but implementation of this method still lags behind the evidence base.
What might this study add?
- These studies demonstrate the effectiveness and safety of iFR-guided PCI in patients with stable multilevel and diffuse coronary artery disease.
- The use of iFR allowed for a 32% reduction in the number of stented lesions by eliminating PCI for functionally insignificant stenoses, with comparable long-term outcomes to traditional PCI without MRC.
- According to univariate regression analysis, physiologically diffuse and combined types of lesions were associated with a six-fold increase in the odds of not achieving the optimal iFR index (≥0,90) relative to the local type.
Aim. To compare the immediate and long-term outcomes of percutaneous coronary intervention (PCI) with and without instantaneous wave-free ratio (iFR) monitoring in patients with diffuse and multilevel coronary artery disease (CAD).
Material and methods. The study prospectively enrolled 100 patients who underwent PCI for stable CAD with diffuse and/or multilevel involvement of target coronary artery. Comparison group was retrospectively matched using a propensity score matching. The study group had iFR-guided PCI (n=100), while the comparison group — standard PCI without iFR monitoring (n=100). Long-term outcomes were assessed in 198 (99,0%) patients.
Results. The study group had a lower number of implanted stents (1,2±0,4 vs 1,6±0,5; p<0,001) and a lower length of stented segments (45,4±14,1 vs 58,7±15,9 mm; p<0,001). The use of iFR monitoring reduced the number of stenoses treated with PCI by 32%. Diffuse involvement was associated with a 6-fold increase in the odds of failing to achieve an iFR ≥0,9 compared to local changes (odds ratio (OR) 6,11; 95% CI 1,44-25,92). Both groups had comparable 12-month risk of achieving the composite endpoint (hazard ratio (HR) 0,51; 95% CI 0,17-1,59; p=0,2460).
Conclusion. In patients with diffuse and multilevel coronary artery disease (CAD), iFR-guided PCI allows for a reduction in the number and length of implanted stents by eliminating the need for stenting functionally insignificant stenoses, with comparable 12-month survival to standard PCI.
What is already known about the subject?
- Carotid stenosis is often associated with hypertension, but the relationship between cerebrovascular hemodynamics and systemic blood pressure (BP) has been poorly studied.
- After carotid endarterectomy and stenting, a transient BP decrease associated with activation of carotid sinus baroreceptors is often observed.
- Most published studies evaluate this effect in the short term and do not take into account the anatomical features of cerebral collateral circulation and the severity of stenosis.
What might this study add?
- It has been shown that a sustained BP reduction after carotid stenting is maintained for 12 months and is observed in almost half (46,6%) of patients.
- An incomplete circle of Willis, severe stenosis (>80%), and intraoperative hypotension are independent predictors of a significant hypotensive effect.
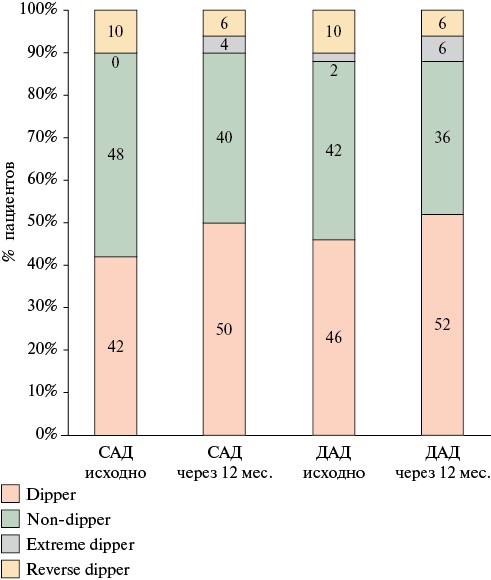
- Carotid stenting promotes the normalization of the circadian BP profile and can be considered a factor in long-term stabilization of systemic hemodynamics.
- The developed algorithm for adjusting antihypertensive therapy before the procedure improves surgical safety and reduces the risk of hyperperfusion syndrome.
Aim. To determine clinical, anatomical, and intraoperative predictors of sustained blood pressure (BP) reduction in patients with ipsilateral internal carotid artery stenosis after carotid artery stenting (CAS).
Material and methods. This single-center prospective study included 178 patients who underwent CAS between 2018 and 2022. All patients underwent clinical BP measurements and ambulatory 24-hour BP monitoring (ABPM) before the [procedure and after 12 months. A sustained hypotensive response was defined as a reduction in average 24-hour systolic/diastolic BP ≥10/5 mm Hg, as measured by ABPM. Anatomical (stenosis degree, plaque morphology, circle of Willis structure, etc.), anthropometric and clinical parameters (age, sex, comorbidities, etc.), as well as intraoperative factors (hypotension, bradycardia, dilation, etc.) were studied.
Results. At baseline, hypertension was detected in 98,6% of patients, while target BP values were achieved in only 28,4%. A significant decrease in office BP was observed as early as 24 hours after CAS (systolic BP 157®114 mm Hg, diastolic BP 87®64 mm Hg; p<0,001). According to ABPM data, after 1-year follow-up, an average decrease in 24-hour BP of 12/9 mm Hg was recorded (p<0,001). A persistent BP reduction ≥10/5 mm Hg was observed in 46,6% of patients. In a multivariate analysis, independent predictors of persistent BP reduction were a incomplete circle of Willis (odds ratio (OR) 3,71; p=0,007), a stenosis >80% (OR 1,06; p=0,033), and intraoperative hypotension (OR 2,42; p=0,022). The number of antihypertensive medications taken by patients did not change statistically, but in 12 cases, the possibility of dosage reduction was noted. The circadian BP profile improved after the procedure (an increase in the proportion of "dipper" patients).
Conclusion. A persistent BP reduction after CAS was observed in almost half of patients with ipsilateral internal carotid artery stenosis. The severity of the hypotensive response is determined by cerebral circulation anatomy (disconnected structure of the circle of Willis), stenosis degree, and intraoperative reactions of the carotid sinus. These factors can be used to predict the hemodynamic response and optimize patient management after CAS.
ISCHEMIC STROKE
What is already known about the subject?
- Atrial fibrillation (AF) is a common cause of cardioembolic ischemic stroke (IS).
- The proportion of patients with AF among patients referred to the 2ndstage of rehabilitation after IS is lower than the proportion of patients with AF during hospitalization after IS.
What might this study add?
- When undergoing mechanotherapy as part of a rehabilitation program, patients with AF demonstrated significantly lower exercise tolerance compared to patients with sinus rhythm.
- Permanent AF partially limits the effectiveness of a 12-day mechanotherapy course as follows: patients achieved an increase in distance, but an increase in power was not achieved.
- Hemodynamic parameters during exercise did not limit training in patients with sinus rhythm and AF.
- Mechanotherapy as part of a post-ischemic stroke rehabilitation program, individualized by intensity and duration of exercise, did not provoke arrhythmia attacks in patients with paroxysmal AF.
Aim. To study hemodynamic characteristics and exercise tolerance during mechanotherapy in patients after ischemic stroke (IS).
Material and methods. The study included 80 patients after IS. Mean age was 61,0±10,5 years, while the duration of ischemic stroke — 13,1±8,5 months. Rehabilitation routing score was 4. Fifty patients have sinus rhythm, while 10 — paroxysmal atrial fibrillation (AF), and 20 — permanent AF. According to Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification, there were 21 patients with atherothrombotic stroke, 30 patients with cardioembolic stroke, 29 patients with stroke of unknown etiology. The following examinations were performed: echocardiography with assessment of left ventricular (LV) global longitudinal strain (GLS), blood test with assessment of N-terminal probrain natriuretic peptide (NT-proBNP). Mechanotherapy was performed daily on a Reck MOTOmed muvi simulator (Germany), with hemodynamic assessment during training on days 1 and 12.
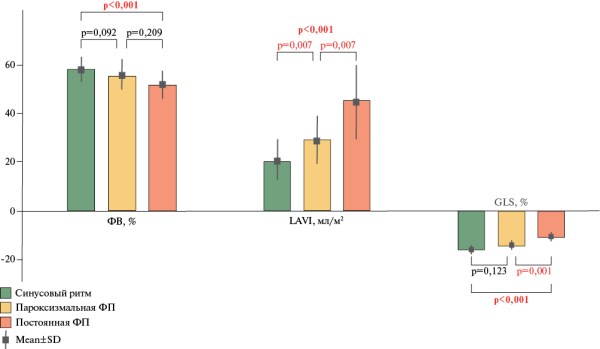
Results. Patients with AF, compared with patients in sinus rhythm, were significantly older (65,7±7,2 vs, 58,0±11,2 years; p=0,002) and had higher NTproBNP levels (192,1 [30,3; 282,2] vs, 15,7 [0; 16,2] pg/ml; p<0,001). In patients with sinus rhythm, compared with patients with permanent AF, the LV ejection fraction was higher — 59,4±4,8 vs 52,7±6,6% (p<0,001), the left atrial volume index was lower — 20,2±7,9 vs 45,0±15,6 ml/min (p<0,001), the LV GLS in absolute values was higher — -16,4±2,0 vs -11,7±2,5% (p<0,001). On the 1st day of mechanotherapy, patients with sinus rhythm demonstrate a greater exercise distance and a higher value of maximum oxygen consumption compared with patients with permanent AF. By the 12th day of rehabilitation, a significant increase in exercise distance was observed in both groups as follows: in sinus rhythm, 1,9±0,9 km vs 2,4±0,9 km (p<0,001), and in persistent AF, 1,3±0,5 km vs 1,8±0,9 km (p=0,005). No clinically significant hemodynamic disturbances were observed during mechanotherapy in any patient, regardless of AF.
Conclusion. During mechanotherapy, patients with AF demonstrated significantly lower exercise tolerance compared to patients with sinus rhythm. Persistent AF partially limited the effectiveness of mechanotherapy: by the 12th day of training, patients achieved an increase in distance, but no increase in power was achieved. Hemodynamic parameters during exercise did not limit training in either patients with sinus rhythm or AF. Mechanotherapy as part of an individualized rehabilitation program after IS did not provoke arrhythmia attacks in patients with paroxysmal AF.
RISK EVALUATION
What is already known about the subject?
- Previously, conflicting results were obtained regarding the association between left atrial reservoir strain (LASr), left ventricular (LV) diastolic function, and age in healthy volunteers.
What might this study add?
- The components of DF — early diastolic mitral annular velocity, components of left atrial (LA) phase strain and transmitral flow velocity — undergo consistent changes with increasing age (from young to middle-aged), while in case of maintaining a normal LV diastolic function, they can be considered a physiological pattern.
- The median of normal LASr values for ages 18-60 years was 37,1%, ages ≤40 years — 38,5%, ages >40 years — 36,2%.
Aim. To investigate the relationship between phase left atrial (LA) strain components using the speckle tracking echocardiography (STE), traditional parameters of left ventricular diastolic function, and age in male volunteers without cardiovascular disease.
Material and methods. Data from 331 male volunteers was analyzed. The study included 167 volunteers (mean age 40,7±7,9 years) without cardiovascular disease or obesity. Group I (n=86) included individuals aged ≤40 years; group II (n=81) >40 years. STE was used to assess left atrial reservoir strain (LASr).
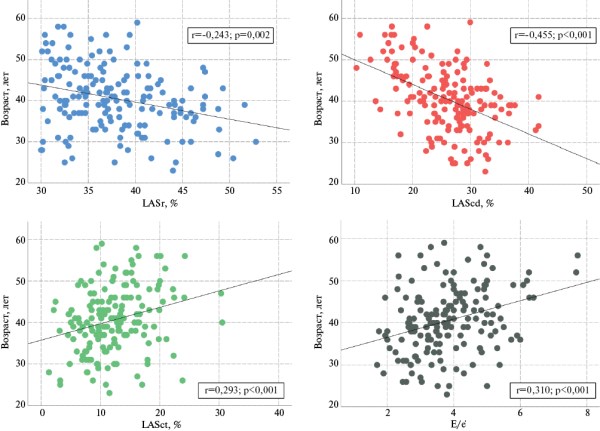
Results. According to the correlation analysis, in the general group, relationships were found between age and LASr (r=-0,243; p=0,002), age and left atrial conduit strain (LAScd) (r=-0,455; p<0,001), age and left atrial contractile strain (r=0,293; p<0,001), and age and left ventricular filling pressure (E/e’) (r=0,310; p<0,001). According to logistic regression, the complex of LAScd (odds ratio (OR) 0,917; 95% confidence interval (CI): 0,863-0,974; p=0,005), early diastolic velocity of the septal part of the mitral annulus (OR 0,747; 95% CI: 0,6200,900; p=0,002) and peak transmitral flow velocity A (OR 1,043; 95% CI: 1,011-1,076; p=0,008) was independently associated with age >40 years. In the ROC analysis, the sensitivity and specificity of the model were 76,5 and 70,9%, respectively (area under the ROC curve (AUC)=0,783; p<0,001).
Conclusion. In male volunteers without cardiovascular disease, an association between traditional and modern measures of diastolic function and age was found. The median normal LASr values for ages 18-60 years was 37,1%, for ages ≤40 years — 38,5%, and for ages >40 years — 36,2%.
CLINICAL CASES
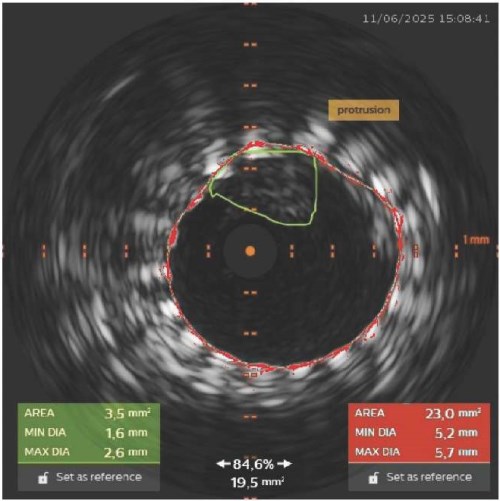
- The use of intravascular ultrasound (IVUS) enabled the timely diagnosis of plaque protrusion through a stent, which was not visible angiographically.
- Intraoperative IVUS monitoring enabled individualized treatment decisions and stroke prevention.
- IVUS confirmed protrusion resolution and adequate stent adaptation after a series of balloon dilations.
- The presented case highlights the strategic importance of IVUS in the safe performance of carotid stenting.
Carotid angioplasty with stenting (CAS) is an alternative to surgery in patients with high surgical risk after carotid endarectomy. According to the large randomized controlled trial Carotid Revascularization Endart-erectomy versus Stenting (CREST), there are no significant differences in the rates of stroke, myocardial infarction, or death in the long-term follow-up between the CAS and carotid endarectomy groups. However,a significant number of complications in the CAS group are associated with the periprocedural period. The safety of CAS directly depends on the technical success of the procedure and minimizing the risk of cerebral embolism. Despite the use of embolic protection in 100% of cases, stroke prevention remains a pressing issue. A clinical case demonstrates the impact of intraoperative intravascular ultrasound (IVUS) on interventional tactics and complication prevention in CAS, and an algorithm for managing intraprocedural plaque protrusion is proposed.
This case confirms that IVUS is not simply a diagnostic tool, but a strategic tool that enables individualized treatment at all CAS stages. Routine use of IVUS for plaque morphology assessment, intraoperative monitoring, and complication management can significantly improve procedural safety. A management algorithm for patients with plaque protrusion is proposed.
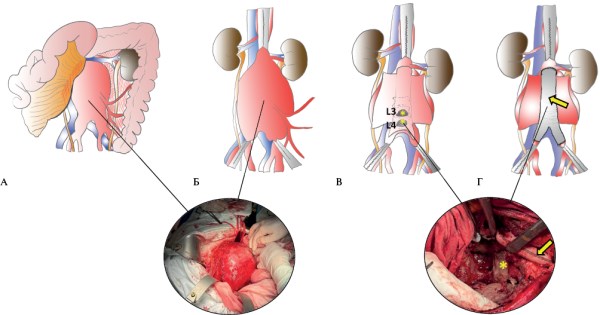
- This article presents a rare case of successful surgical reconstruction of a giant ruptured abdominal aortic aneurysm, characterized by a high mortality risk and technical complexity of the procedure.
- The technical complexity of the surgical intervention in this case was due to the juxtarenal extension of a giant abdominal aortic aneurysm, the absence of a posterior wall of the aneurysm, and lumbar vertebral body destruction as a result of prolonged compression.
- A favorable outcome in the surgical treatment of ruptured abdominal aortic aneurysms depends on the timely provision of care by a highly qualified multidisciplinary team of specialists, as well as modern equipment in the operating room and intensive care unit.
In the era of national screening programs and the widespread availability of vascular ultrasound and multislice computed tomography, a giant abdominal aortic aneurysm with a diameter greater than 10 cm is a rare clinical finding. Delayed surgical treatment of a giant abdominal aneurysm leads to its rupture, with a mortality rate of <90%. Furthermore, performing both open and endovascular reconstructions presents a complex technical challenge for the treatment of this patient population. This article presents a case of successful aneurysmectomy in a patient with a giant ruptured juxtarenal abdominal aortic aneurysm. This case is considered unique due to the rarity of this pathology and the successful surgical outcome. This case highlights the importance of timely diagnosis, surgical intervention, and a multidisciplinary approach to achieving a favorable outcome in patients with a ruptured giant abdominal aortic aneurysm.
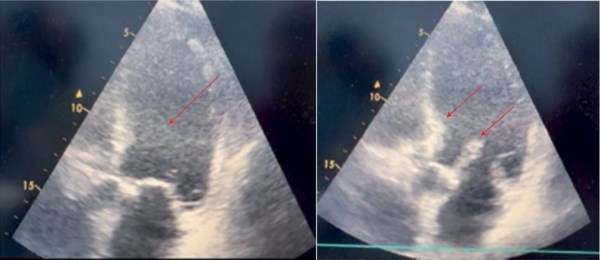
- Diagnosis of bilateral pneumonia in obese patients with heart failure (HF) with reduced ejection fraction (HFrEF) requires apprehensive attitude, as symptoms may mimic acute decompensated HF.
- The results of a 15-week follow-up of a 60-year-old patient with bilateral pneumonia, obesity, HFrEF, hypertension, subclinical hypothyroidism, urolithiasis, and other risk factors for cardiovascular events are presented.
- Despite physical signs of pneumonia, the examination did not reveal typical laboratory or radiographic markers of acute inflammation. A comprehensive clinical, diagnostic, and therapeutic approach ensured timely diagnosis, disappearance of pneumonia symptoms and improvement of left ventricular contractility.
Obesity is a widespread chronic disease of the 21st century, characterized by excess accumulation of adipose tissue and weight gain. These patients have a significantly increased risk of cardiovascular disease and vulnerability to respiratory infections. Cardiorespiratory complications remain the leading causes of death. The combination of bilateral pneumonia (BP) and heart failure (HF), developing in the context of obesity, significantly worsens the prognosis.
Brief description. This case presents describes a 60-year-old patient with obesity, bilateral pneumonia, HF, and hypertension. The main complaints were shortness of breath on exertion, cough with nummular sputum, and palpitations. The history included myocardial infarction. Body mass index was 36,8 kg/m2, oxygen saturation (SpO2) — 86-89%. In addition, there were high respiratory rate, moderate cyanosis, reduced breath sounds, dry and wet rales. Blood pressure was 140/80 mm Hg, heart rate — 100 beats/min. Computed tomography revealed infiltrative and reticular changes in both lungs. Echocardiography revealed a decrease in the left ventricular ejection fraction to 20% and dilation. Elevated brain natriuretic peptide levels were noted. The diagnosis of bilateral pneumonia was established based on clinical and paraclinical data. Treatment was administered according to clinical guidelines. After 15 weeks, computed tomography showed following improvements: improved left ventricular (LV) contractility, decreased LV size. However, there was a decrease in glomerular filtration rate.
Conclusion. This case reflects the atypical onset of bilateral pneumonia in a patient with obesity and HF: the disease manifested primarily with physical and imaging signs in the absence of laboratory markers of inflammation. This emphasizes the need for advanced diagnostics and individualized therapy, as the presence of pneumonia increases the risk of renal and cardiorespiratory complications.
REVIEW ARTICLES
What is already known about the subject?
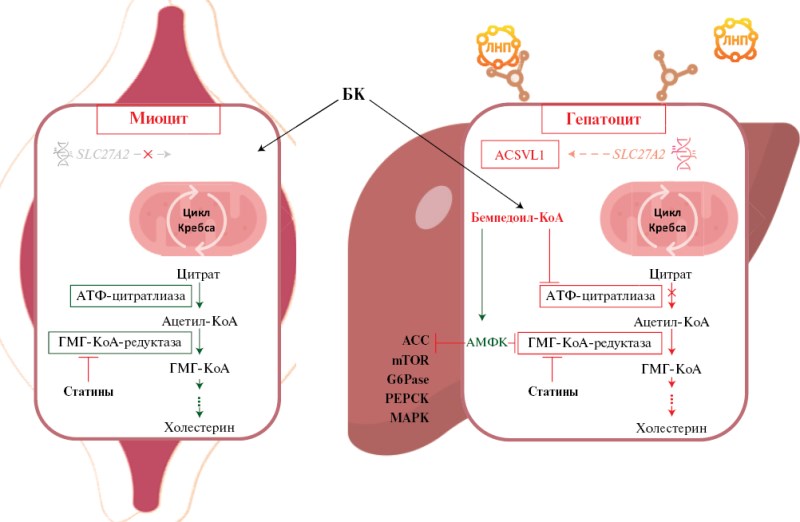
- Bempedoic acid (BA) is the first oral adenosine triphosphate-citrate lyase inhibitor with a tissue-specific mechanism of action.
- The drug provides a significant reduction in low-density lipoprotein cholesterol and high-sensitivity C-reactive protein levels.
- BA therapy is associated with a 13% reduction in the risk of major cardiovascular events.
What might this study add?
- Current data on the clinical efficacy of BA in monotherapy and various combinations are summarized.
- The safety profile of BA is analyzed.
- Current information on the pleiotropic effects of BA and its place in current international and national clinical guidelines is summarized.
The study aim was to provide an overview of current data on the mechanism of action, clinical efficacy, and safety of bempedoic acid (BA) as a lipid-lowering drug.
The methodological approaches included a literature search of PubMed, Web of Science, and Scopus for studies published before December 19, 2025. The review included randomized controlled trials (RCTs) evaluating the efficacy and safety of BA compared to placebo in patients with hypercholesterolemia, including the Cholesterol Lowering via Bempedoic Acid, an ACL-Inhibiting Regimen (CLEAR) series of studies. Data from metaanalyses and other clinical trials were also considered.
The obtained results demonstrate that BA is the first oral adenosine triphosphate citrate lyase inhibitor, which plays an important role in the treatment of hypercholesterolemia. Due to tissue-specific activation mechanism, BA can be used in patients with statin intolerance. RCT data have demonstrated that when added to maximum-tolerated doses of statins, BA provides an additional reduction in low-density lipoprotein cholesterol (LDL-C) by 15-23%. In monotherapy, in patients with statin intolerance, LDL-C reduction reaches 23-27%. The combination of BA and ezetimibe demonstrated a reduction in LDL-C by 38-45%, and with high doses of statins, BA, and ezetimibe, a reduction of 68%. BA therapy also helps reduce high-sensitivity C-reactive protein levels by 19-32%. Longterm BA use is associated with a 13% reduction in the risk of cardiovascular events compared to placebo, with a favorable safety profile. A subanalysis of the CLEAR studies showed that BA does not increase the incidence of type 2 diabetes.
Thus, BA is an effective and safe lipid-lowering agent that reduces the risk of major cardiovascular events and can be used both as monotherapy and in combination with other lipid-lowering agents.
What is already known about the subject?
- The problem of timely detection of anthracycline-induced cardiovascular toxicity is a pressing concern for cardio-oncology specialists.
- The ongoing issue of the occurrence of negative effects of antitumor therapy in cancer patients requires the use of novel diagnostic methods.
What might this study add?
- Modern diagnostic methods allow for a comprehensive approach to identifying manifestations of cardiovascular toxicity, including laboratory (determining the level of cardiac and genetic markers) and radiological diagnostics.
- Among diagnostic radiology methods for the cardiovascular system, coronary computed tomography angiography and cardiac magnetic resonance imaging proven their effectiveness.
The emerging problem of cardiovascular toxicity associated with antitumor therapy raises the question of timely diagnosis of its early manifestations. To address this issue, a literature review was conducted on an integrated approach to diagnosing early manifestations of cardiovascular toxicity induced by anthracycline antibiotics, including genetic marker testing, coronary computed tomography angiography (CCTA), and cardiac magnetic resonance imaging.
METHODICAL GUIDELINES

These guidelines describe the management of outpatient monitoring of patients with stable coronary artery disease by a general practitioner and include modern approaches to diagnosis — clinical and paraclinical methods — as well as treatment and prevention of complications.
These guidelines will enable physicians to make informed clinical decisions within outpatient monitoring for patients with stable coronary artery disease based on the related algorithm presented (examinations, consultations).
The guidelines are intended for general practitioners, family doctors, as well as for mid-level health providers working with the above-mentioned doctors, for paramedics performing the doctor functions regarding organizing and conducting outpatient follow-up. These guidelines can be used by healthcare executives, heads of primary care facilities, and their departments.

ISSN 2619-0125 (Online)
















































